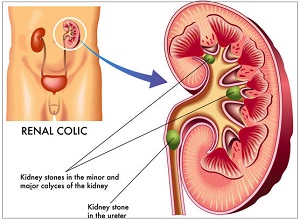
Procedure– A small 2 to 3 mm diameter long slender endoscope is introduced through the urethra into the ureter and the stone is fragmented or removed. 99% stones can be cleared with good success rate. 1.Limitation due to Anotomical constraints, stones migrating up. 2. Miniature or flexible URS may be required 3. C-Arm guidance.
Blader stones
1. Almost any stone can be done Endoscopically. 2. Hospital stay less than a day. 3.No pain. 4.Small stones done on OPD basis under LOCAL NAESTHESIA A.Mauer Mayer stone punch. 5.Blader stone sheath / Nephroscope. 6.Success rate almost 100% 7.Complication rate almost 0%
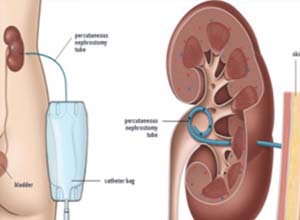
Antegrade PCNL
1. Large / Hard stones 2. Stones not accessible to URS. 3. Stone migration during URS. 4. Success rate very high 5. Push Bang ESWL 6. Ureterolithotomy, Retroperitoneo scopy, Laparo scopy etc.
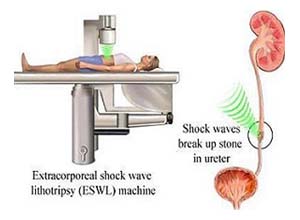
ESWL
EXTRACORPOREAL SHOCKWAVE LITHOTRIPSY Credit for the invention of LITHOTRIPSY goes to Doenier.It is a procedure wherein NO Anaesthasia is required and it is not at all an operation. The Urologist does not even touch the patient. The patient just lies down on the Lithroscopy table, a 6 inches baloon touches the Lion and Soundwaves hit the body which feels like strong tapping on the skin. It is done on the OPD basis and the patient is called back for subsequent sittings depending upon the size and the hardness of the stone. 1. Success rate 95% 2. No admission 3. Non Invasive 4. No Anaesthesia 5. Age no bar 6. Minimal side effects
Advantage of Dornier ESWL
Totally non invasive-no incision or passage of catheters or scopes
No anaesthesia
No pain
OPD basis treatment
Safe for all age groups Upto 3cm stones can be cleared
Best choice for poor risk & recurrent stone formers.
Few cases done at Pramodini Urology Foundation
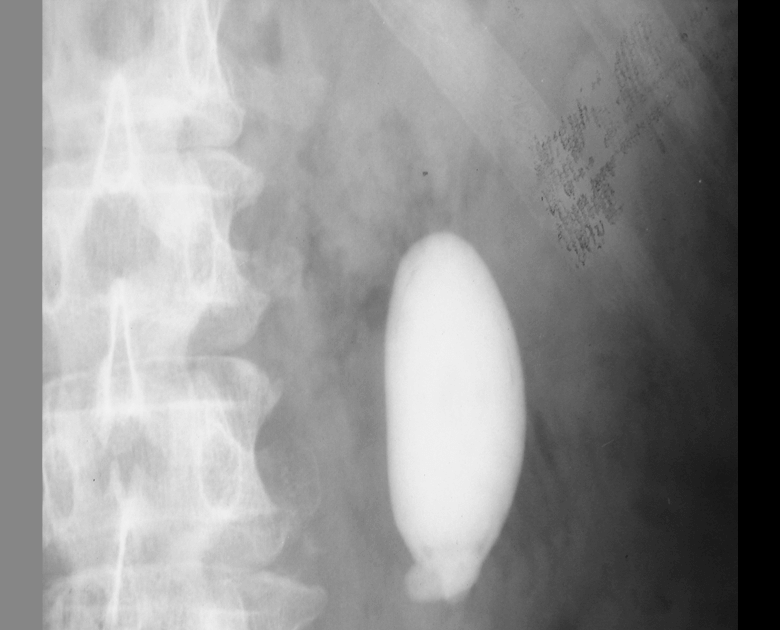
Upper 1/3rd Uteric Stone
Afer 5 minutes of ESWL
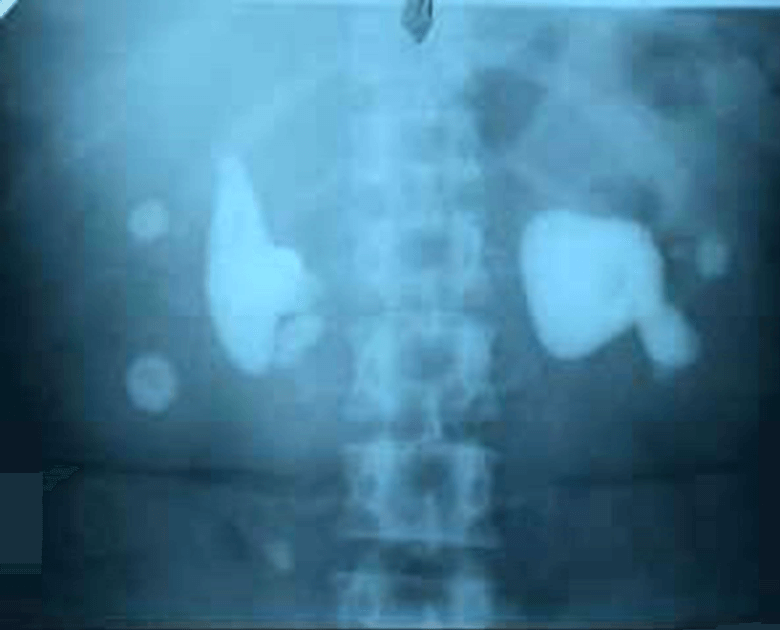
Afer 10 minutes of ESWL
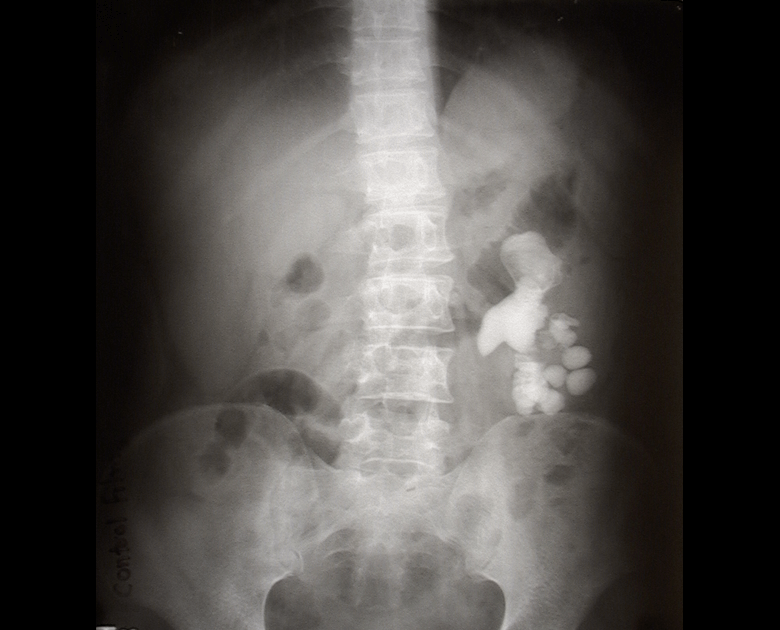
Large Renal Stone
Afer 20 minutes of ESWL
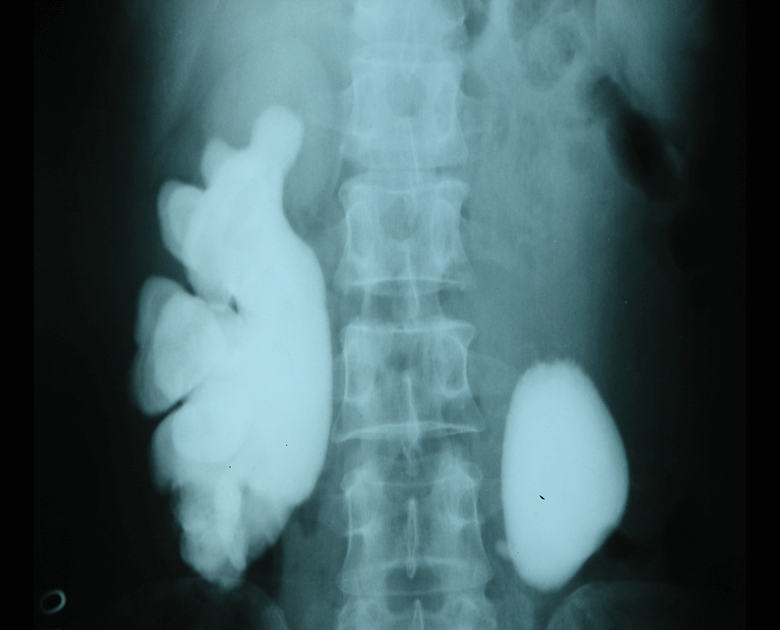
At the end of first sitting of ESWL
When Patient come for 2nd sitting after 1 week
At the end of the 2nd sitting of ESWL
Bilateral ESWL done on 7 months old child
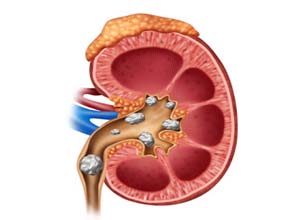
PCNL
Pramodini urology foundation boasts about performing more than 5000 pcnls till date.
The stone size varying from 1 cm till 10 cm and age varyng from 1 year till 87 years. 19 french drasden (richard wolf) nephroscope allows access to all calyces thereby improving stone clearance rates.
As these specialized endourological procedures are being done at this institute, apart from routine procedures like turp, ureteroscopies, bladder stones etc, pramodini urology foundation has become one of the leading institutes in endourology in india.
We have added mini perc (4-5 mm hole) and ultra mini perc (2-3 mm hole) to clear kidney stones through very small punctures using lasers. These specialized endourological procedures are being done at this institute, apart from routine procedures like turp, ureteroscopies, bladder stones etc. Prabodhini urology foundation has become one of the best leading institutes in endourology in india.
We are also performing number of reconstructive urological surgeries like end to end – buccal mucosal graft urethroplasties – pyeloplasties lap as well as open, ureteric reimplantations, hypospadias repairs etc.
With more than 10,000 operations to it’s credit, pramodini urology foundation is eying not only national but international standards.
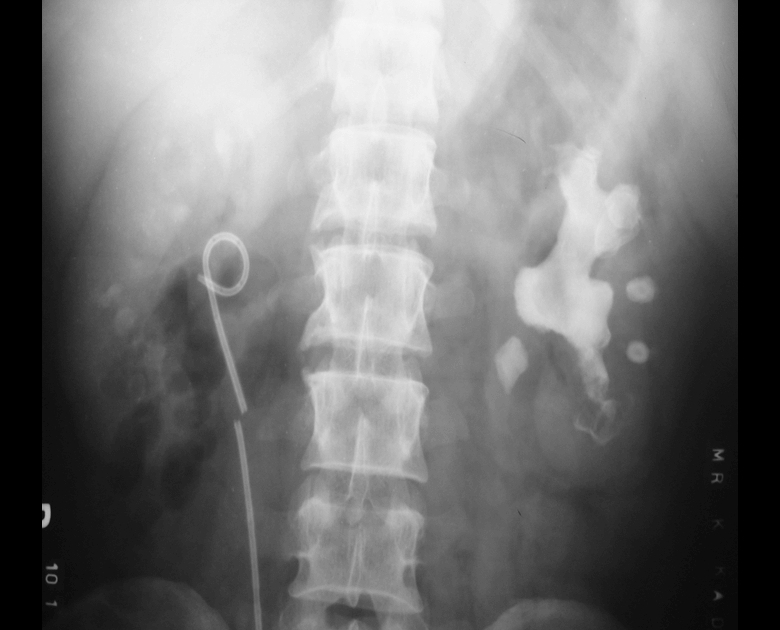
Patient of Broken stent with left staghorn Stone cleared by PCNL
Left Large Renal Stone Cleared by PCNL
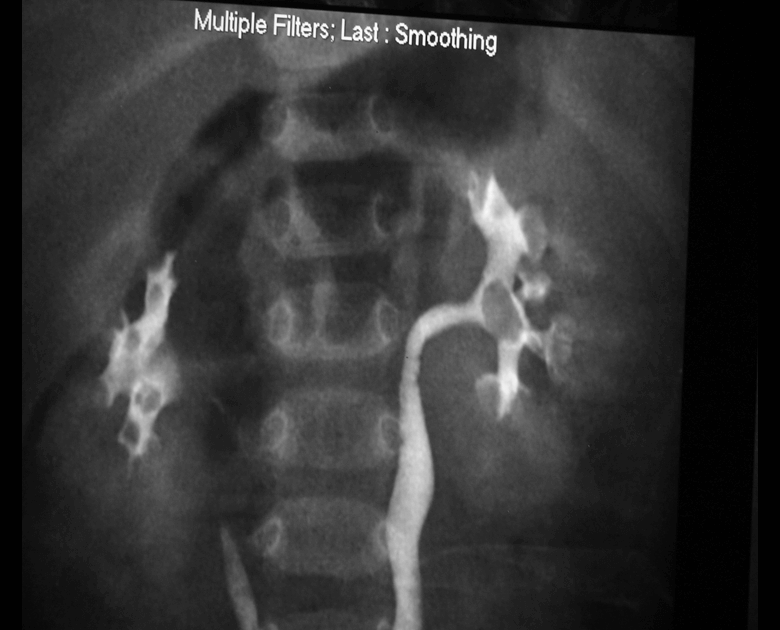
Bilateral staghorn Renal Stone – Single Sitting Bilateral PCNL – Total Clarence
Staghorn Stone cleared by PCNL
17cm Large Staghorn Rt Renal Stone Cleared by Pycloithotomy
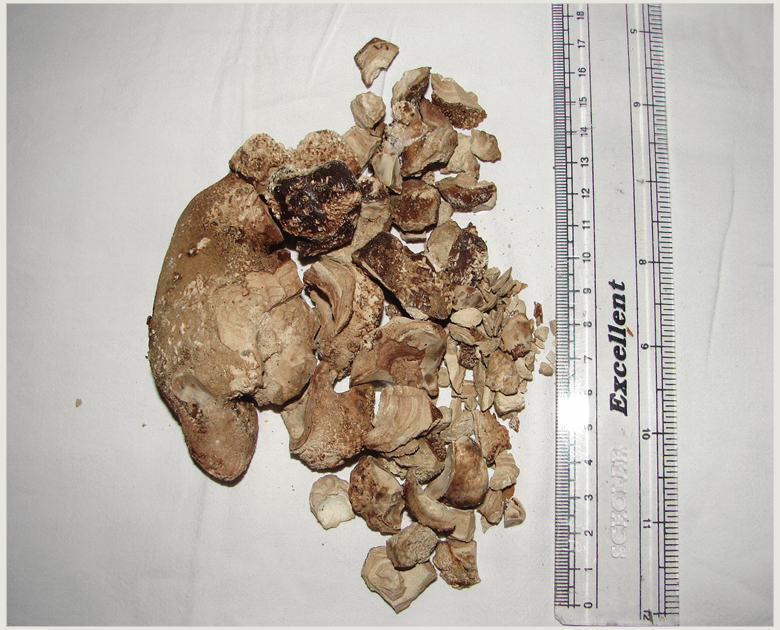
Extracted Stones
Mini-PCNL
Minimal invasive percutaneous nephrolitholapaxy(so-called Mini-PCNL) The minimal invasive percutaneous nephrolitholapaxy, abbreviated Mini-PCNL, is an endoscopic procedure to remove kidney stones. It is used for larger kidney stones (>1.5cm) or if other therapy methods, e.g. shock wave treatment (ESWT) or flexible ureterorenoscopy, have not been or do not seem successful due to anatomic particularities of the pelvicalyceal system.
A special miniaturised instrument is used for Mini-PCNL. The surgery takes place under general anaesthesia. After contrast medium imaging of the kidney tract on the effected side, the kidney is punctured directly through the skin in the area of the flank. The puncture is controlled via fluoroscopy and ultrasound. After carefully dilating (using a bougie) of the puncture canal, the endoscope is inserted into the kidney. Using a special laser, the kidney stones are then broken up and washed out while a direct view of the operation is provided. At the end of surgery, a catheter (hose), a so-called renal fistula, is placed in the kidney to secure the outward urine flow. This catheter can generally be removed without any pain a few days after surgery.
Mini-PCNL constitutes an effective and very safe method to treat kidney stones. Depending on the size of the stone, repeated surgery is only very rarely required. Generally, the patient is immediately “stone-free”. The use of small instruments makes Mini-PCNL a low-risk procedure. Severe complications like heavy bleeding are extremely rare and treatable.
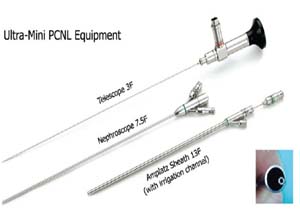
Ultra-mini PCNL
Ultra-mini-percutaneous nephrolithotomy Since the introduction of percutaneous nephrolithotomy (PCNL) there have been various modifications to improve success rates. The overall complication rate of PCNL can be up to 83%, which can be minimised by accurate patient selection and careful postoperative follow-up. One of the most important differencesbetween the various PCNL techniques is the size of renal access (and the required specialised equipment), which contributes to the broad spectrum of complications and outcomes. Today, PCNL techniques include: standard PCNL (S-PCNL), mini-PCNL (also called mini-perc), ultra-mini-PCNL (UM-PCNL), and the recently introduced micro-PCNL. S-PCNL is the standard procedure in the treatment of renal and upper ureteric stones using a 28–30-F ureteroscope. The mini-PCNL (mini-perc) was first introduced by Helal et al.in 1997 using a 10-F paediatric cystoscope in children, which reduced the complications of the standard method. This technique was shown to have a stone-free rate (SFR) of 85% with minimal morbidity in young children. Furthermore, it was shown that it could be used for all kinds of upper tract stones. In UM-PCNL, the adult size ureteroscope is replaced with a nephroscope with a smaller metal sheath. The last procedure is micro-PCNL using unique equipment as well. In micro-PCNL, the 4.85-F needle reaches the collecting system under direct vision, and renal access and PCNL are performed in a single step
RIRS
RIRS (retrograde intrarenal surgery) RIRS (retrograde intrarenal surgery):Retrograde intrarenal surgery (RIRS) is a procedure for doing surgery within the kidney using a viewing tube called a fiberoptic endoscope. In RIRS the scope is placed through the urethra (the urinary opening) into the bladder and then through the ureter into the urine-collecting part of the kidney. The scope thus is moved retrograde (up the urinary tract system) to within the kidney (intrarenal). RIRS may be done to remove a stone. The stone is seen through the scope and can then be manipulated or crushed by an ultrasound probe or evaporated by a laser probe or grabbed by small forceps, etc. RIRS is performed by a specialist, an urologist (endourologist) with special expertise in RIRS. The procedure is usually done under general or spinal anesthesia. The advantages of RIRS over open surgery include a quicker solution of the problem, the elimination of prolonged pain after surgery, and much faster recovery.